In brief: Diabetic foot results from the combination of nerve damage (neuropathy) and artery narrowing in people with diabetes, leading to non-healing wounds. With blood sugar control, wound care and opening blocked arteries, amputation can often be prevented.
Why Do Diabetic Foot Wounds Not Heal?
Three problems combine: loss of sensation (neuropathy), reduced blood supply (peripheral artery disease) and infection. Without enough blood flow, the wound cannot get the oxygen needed to heal.
Treatment and Limb Salvage
- Blood sugar control — the basis of healing
- Wound care and removal of dead tissue (debridement)
- Offloading pressure with suitable footwear
- Opening blocked arteries (revascularisation)
- Treating infection when present
Amputation is considered only when tissue death is extensive or infection is life-threatening; with early intervention the limb can often be saved.
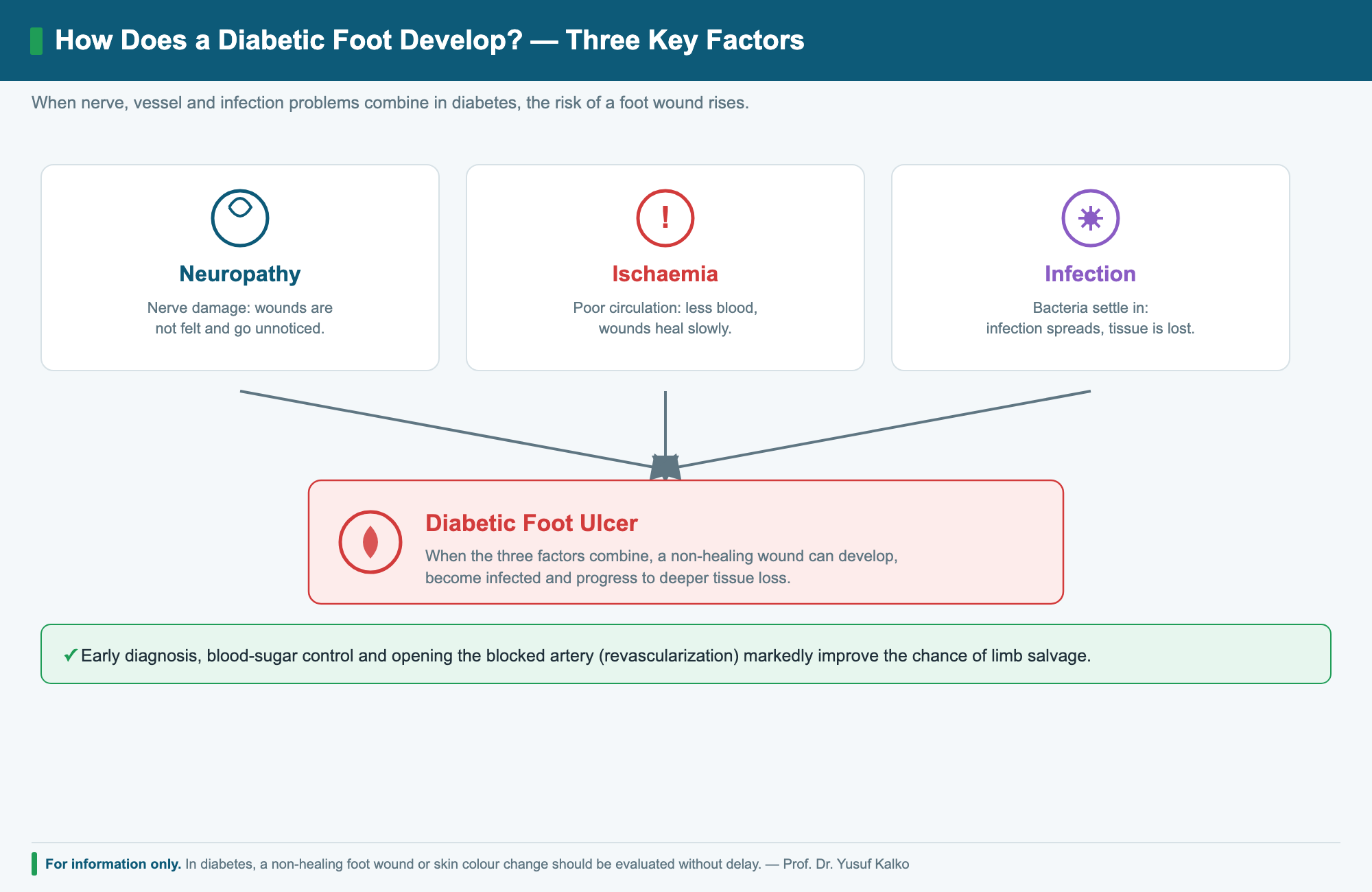
How Does a Diabetic Foot Develop?
Persistently high blood sugar gradually damages both the nerves and the arteries. Because of neuropathy, pain and touch sensation in the foot are reduced, so a tight shoe, a small stone or a minor cut may go unnoticed and turn into a wound under pressure. Because of poor circulation (ischaemia), not enough blood, oxygen and immune cells reach the area, so the wound heals slowly. Once the skin is broken, bacteria settle easily and infection accelerates the problem. When these three factors come together, a seemingly small wound can quickly deepen into a serious one.
Types of Diabetic Foot
Depending on which factor is dominant, diabetic foot is grouped into three main types, and this distinction helps guide treatment:
- Neuropathic foot: loss of sensation is dominant while circulation is usually preserved; wounds are often painless and appear over pressure points such as the sole.
- Ischaemic foot: artery narrowing is dominant; the foot is cold, pale and painful, and wounds struggle to heal.
- Neuro-ischaemic foot: both nerve damage and poor circulation are present together — the most common and highest-risk type.
Symptoms of Diabetic Foot
- Numbness, tingling or loss of sensation in the foot
- Non-healing wounds, cracks or wounds beneath calluses
- Colour change, darkening or coldness of the foot
- Swelling, discharge, bad odour or redness (signs of infection)
- Leg pain on walking (associated artery narrowing)
Because of reduced sensation, these wounds can be painless and therefore noticed late. For this reason, regular foot checks matter even when no symptoms are felt.
Stages of Diabetic Foot (Wagner Classification)
Diabetic foot wounds are commonly graded using the Wagner classification, which describes the depth and severity of the wound and helps guide the treatment plan:
- Grade 0: no open wound, but a foot at risk (calluses, deformity, dry or cracked skin).
- Grade 1: a superficial wound (ulcer) involving only the skin.
- Grade 2: a deeper wound that may extend to tendon, capsule or joint.
- Grade 3: deep infection, abscess or bone infection (osteomyelitis).
- Grade 4: localised gangrene (toe or forefoot).
- Grade 5: extensive gangrene affecting most of the foot.
The earlier the stage, the higher the chance of saving the limb — which is why prompt assessment is so important.
Causes and Risk Factors
The most decisive factor in developing a diabetic foot is long-standing high blood sugar. Accompanying risk factors make the picture worse:
- Long-standing, poorly controlled high blood sugar
- Peripheral artery disease (blocked leg arteries)
- Smoking
- Foot deformities, unsuitable footwear and calluses
- Poor vision and limited mobility (difficulty checking the feet)
- A previous foot wound or tissue loss
Possible Complications
A neglected or late-treated diabetic foot wound can progress to the following serious problems:
- Spreading infection: inflammation spreading into soft tissue (cellulitis), abscess and, in severe cases, a body-wide infection (sepsis).
- Bone infection (osteomyelitis): infection reaching the underlying bone, which is harder to treat.
- Charcot foot: breakdown and deformity of the bone and joint structure due to nerve damage.
- Tissue and limb loss: risk of amputation when gangrene and infection cannot be brought under control.
How Diabetic Foot Is Diagnosed
In diagnosis, measuring the blood flow to the foot and assessing infection are as important as evaluating the wound itself:
- Examination: assessment of wound depth, pulses, sensation and signs of infection.
- Vascular imaging: colour Doppler ultrasound and, where needed, CT or MR angiography to locate and grade any blockage.
- Laboratory tests and imaging: investigation of infection and bone involvement (osteomyelitis).
- Treatment plan: a personalised plan combining artery opening, wound care and infection management.
A Multidisciplinary Treatment Approach
Diabetic foot treatment is not a single procedure; it is a multidisciplinary and individualised process. Its main components are:
- Opening the artery (revascularisation): the blocked artery is reopened to increase blood flow to the foot, using endovascular (balloon/stent), open (bypass) or combined methods. Adequate circulation is the basic requirement for healing.
- Removing dead tissue (debridement): cleaning the wound supports faster healing.
- Infection control: appropriate antibiotic treatment when required.
- Modern wound care: suitable dressings and regular follow-up.
- Offloading pressure: special footwear, insoles or splints that reduce the load on the wounded area.
- Blood sugar and general health management: regulating blood sugar, nutrition and stopping smoking.
Which methods are used, and in which order, depends on the stage of the wound, the state of circulation and the patient’s overall health.
Combined Wound Treatment and Newer Technologies
In infected diabetic foot wounds, the best results come not from a single method but from a combined approach: restoring blood flow to the foot (revascularisation), bringing infection under control and applying modern wound care together. Technologies that may be used in current wound treatment include:
- Negative-pressure wound therapy (vacuum/VAC) to support wound healing
- Advanced wound dressings with regular, controlled changes
- Hyperbaric oxygen therapy in selected cases
- Offloading applications and multidisciplinary follow-up
Recovery and Follow-up
Even after circulation has been improved, diabetic foot wounds can take time to heal and require regular dressing changes and close follow-up. Because the risk of recurrence continues after a wound has closed, foot care and regular check-ups remain important for life. The course of treatment and the outcomes vary from person to person.
Foot Care and Prevention
Most diabetic foot problems can be prevented with appropriate care:
- Check your feet every day (including the soles; use a mirror if needed)
- Moisturise the skin and keep the spaces between the toes dry
- Wear well-fitting, non-pinching shoes and never walk barefoot
- Trim nails carefully and do not cut calluses yourself
- Change socks daily and check inside shoes for foreign objects
- Keep blood sugar under control, stop smoking and attend regular check-ups
When should you see a doctor? People with diabetes should seek assessment without delay if they notice a non-healing wound, colour change, darkening, swelling, redness or loss of sensation in the foot. Do not wait, even if the wound looks small.
Frequently Asked Questions
Can a diabetic foot wound heal?
Yes, in most cases — with blood sugar control, wound care and, when needed, opening the blocked artery so the tissue receives blood again.
When is amputation needed?
Only when tissue death is extensive or infection is life-threatening. Early intervention can often save the limb.
Is this medical advice?
No. This page is for information only; please consult a physician for diagnosis and treatment.
What is diabetic foot?
It is a condition in which nerve damage (neuropathy) and artery narrowing caused by diabetes together make the foot prone to wounds and infection.
Why does a diabetic foot develop?
High blood sugar gradually damages the nerves and arteries; sensation is reduced, circulation worsens, and small wounds can progress unnoticed.
What are the symptoms of diabetic foot?
Numbness or tingling, loss of sensation, coldness, colour change, non-healing wounds and wounds beneath calluses are the main signs.
What is the role of vascular surgery in diabetic foot?
Opening blocked or narrowed arteries to the foot (balloon/stent, bypass or combined methods) can increase blood flow and improve the chance of the wound healing.
Why do diabetic foot wounds heal slowly?
Both reduced circulation and the effect of high blood sugar on immunity and tissue repair cause these wounds to heal slowly.
Which diabetic foot wounds are urgent?
Wounds that grow quickly, smell bad, are accompanied by redness, swelling and fever, or begin to darken (gangrene) require urgent assessment.
Why does early assessment matter?
When circulation is improved and infection is controlled early, the risk of limb loss can be markedly reduced.
How should foot care be managed in diabetes?
Checking the feet daily, moisturising, wearing suitable shoes, trimming nails carefully and avoiding walking barefoot are all important.
Can diabetic foot be prevented?
With good blood sugar control, regular foot care and routine check-ups, many diabetic foot problems can be prevented.
Video — Prof. Dr. Yusuf Kalko
Prof. Dr. Yusuf Kalko explains diabetes management and its impact on the vessels. (Video in Turkish.)
Related
Peripheral Artery Disease · Minimally Invasive Vascular Surgery · Buerger’s Disease
This content is for information purposes only and does not replace a medical consultation. Diagnosis and treatment require an in-person examination. — Cardiovascular Surgeon Prof. Dr. Yusuf Kalko